Haemorrhoids (Piles)
(public version page) Doctors Click here
What are haemorrhoids?
The anal canal is normally lined by specialized mucosal lining called anal cushions. These are formed by a network of elastic fibres with intervening blood vessels. They fill with blood and thus slightly bulge inwards, helping in completely occluding the anal canal during rest. During defaecation, motion passes over them, deflating these anal cushions, which may also move slightly downwards, only to be pulled back in place by the elastic fibres. These cushions are thus exposed constantly to shearing forces when passing a motion.The elastic fibres which pull them back in place can disintegrate with age, especially in people prone to constipation and habitual straining. At that stage these anal cushions remain prolapsed forming haemorrhoids. Haemorrhoids are therefore prolapse (sliding down) of the anal canal lining.
Haemorrhoids are not uncommon during pregnancy and delivery. They are also common in patients with constipation and straining, but can still appear in patients without any of the aforementioned conditions.
Haemorrhoids may be asymptomatic or they may bleed, cause discomfort or protrude outside the anal canal. It is vital that patients do not assume that bleeding from the back passage is because of haemorrhoids. Always seek reassurance regarding the cause of such bleeding from your GP or specialist. Likewise, if long standing haemorrhoids start giving symptoms, beware it is not anal canal cancer masquerading as haemorrhoids (see anal cancer)
Uncomplicated haemorrhoids are soft to touch and generally non palpable and non tender. If you can feel anything in the anal canal (or if there is tenderness), then it is not uncomplicated haemorrhoids.They tend to occur at 3, 7 & 11 O'clock position around the anus, but may occur at other places and may be circumferential. Haemorrhoids may be classified into "degrees"
Treatment options: Tailoring it to individual bottoms!
Haemorrhoids can be treated medically in many early cases, but often require some form of surgical intervention at some point. This may vary between injection, banding or surgery.
The problem is that no two people will have similar problems and thus one can not generalize about treatment. Basically the treatment has to be tailored to the individual patients and only surgeons with an interest in anorectal surgery have sufficient expertise to provide patients with correct advice.
One of the not uncommon mistakes in the surgical treatment of haemorrhoids is that it may be relegated to a junior surgeon, sometimes even without supervision. This is often a misjudgment, since this condition really needs expert assessment to judge how to tailor treatment to a particular patient. Haemorrhoids were not created equal in this world. It is just not possible to use a standard operation in a patient.
Conservative medical treatment
Medical treatment is quite useful in early stages of haemorrhoids & probably helps the vast majority of patients. This involves:
- Avoidance of constipation
- Avoidance of straining at stools
- Increase dietary fiber, eating more fruit and vegetables or fiber rich cereals
- Astringent local applications (creams or suppositories), e.g. xyloproct or proctosedyl. Astringent local applications gives moderate symptomatic relief to symptoms, but are palliative at best.
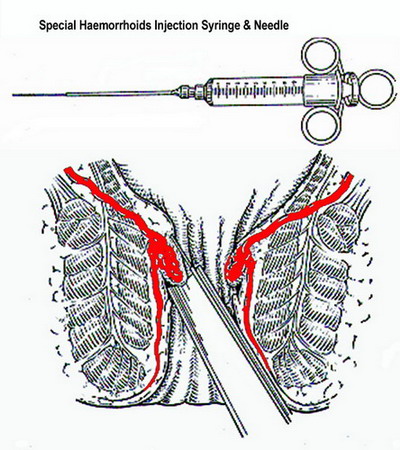
Injection sclerotherapy
Injection sclerotherapy is usually used for treating bleeding internal haemorrhoids, but is not terribly successful in preventing recurrent bleeding in the long term, hence it is becoming less popular with surgeons. It is generally successful in stopping bleeding in the short term. Injecting sclerosing material (usually phenol in almond oil) into haemorrhoids aims at fixing the haemorrhoidal cushions in place, by inducing fibrosis (in the submucosal plane) and thus preventing the haemorrhoids from bulging excessively & sliding down, and decreasing the chance of these being traumatized during defaecation and causing haemorrhoidal symptoms (usually bleeding).
Rubber band ligation
This is a popular, useful and generally very safe method in treatment of haemorrhoids. It involves the insertion of tiny rubber rings around the haemorrhoidal tissue, which strangulate it and cause it to fall off after about 7-10 days, when the patient may notice the passage of some blood with stools. This can be repeated after 4-6 weeks, if need be.

Bands can only be applied on the insensitive internal haemorrhoids, but not on the very sensitive external haemorrhoids (otherwise it is very painful). It is thus mainly indicated in bleeding and prolapsing moderate internal haemorrhoids.
It should not be used in patients with known bleeding disorders or depressed immunity. It may be wise to stop Aspirin, non steroidal ant inflammatory and anticoagulants 1 week before the procedure.
If brisk bleeding occur, report to your doctor. Likewise if pain becomes worse (not better)
after few days, along with fever or retention of urine, you must report immediately to your doctor, this may be symptoms of an infection developing at the sites of banding
Surgery
Surgery remains the mainstay of treatment in many patients. This is especially so in those with large haemorrhoids (prolapsing haemorrhoids), those with acute painful thrombosed (with a clot inside) or those patients with mainly external haemorrhoids. Surgery is performed in 2 completely different ways:
A) The traditional excisional haemorrhoidectomy . This essentially removes the prolapsed haemorrhoidal tissues. It is done in a variety of ways, but there are 2 main excisional techniques: the open technique (Moran-Milligan), where the haemorrhoids are excised and the wounds left open (the favourite method in the UK, when excisional haemorrhoidectomy is done) and the closed technique (Ferguson), where the wounds are sutured (stitched) after excision, which is the method favoured in the USA.
B) PPH (Procedure for Prolapse & Haemorrhoids, Longo procedure) or stapled anopexy. In this method, the haemorrhoidal tissues are not excised, but instead a small 3-4 cm cylinder of the lining of the lower rectum is excised, with the edges stapled together, pulling up the haemorrhoidal tissue from its prolapsed position into a more normal position
It is important not to view these 2 options only as alternatives, because they are also complimentary and with experience, the surgeon can advise patients if traditional haemorrhoidectomy or PPH is best for condition or whether both are equally suitable in his / her case
Traditional haemorrhoidectomy
The importance of experience in this operation can not be over emphasized. Many patients present with lots of haemorrhoids (the so called primary haemorrhoids as well as the smaller daughter haemorrhoids). This present the surgeon with a dilemma, for if he removes too much, he may cause narrowing of the anus. On the other hand removing the right amount of tissue leaving behind daughter haemorrhoids to guard against such narrowing is usually not appreciated by patients, who blame their doctors for doing an inadequate operation. It goes without saying that correction of narrowing is much more difficult than simple excision of such daughter haemorrhoids at a later stage. Experience is also important to safeguard against injury to sphincters (muscles around anus) and inducing incontinence (loss of control of wind or even faeces). Again haemorrhoidectomy needs to be tailored to individual patients's disease.
Postoperative care
After the operation, it is important for patients to stay in the hospital until after the first bowel motion, as the degree of pain in individual patients is unpredictable. Surgeons should ensure that patient can go home in a relatively pain free state, able to pass motions without much discomfort.
One of the recurring problems with patients postoperatively is that they may not follow the surgeon’s advice regarding adequate cleaning and proper use of anaesthetic gels. They usually come complaining of worse pain than when they were in the hospital and are usually amazed by the prompt improvement, one the surgeon re-emphasizes the importance of adequate cleaning and the use of xylocaine gel inside the anus as well as outside it.
The short & long term results of haemorrhoidectomy, are really excellent, with long term relief of symptoms. Again it is important to minimize straining to prevent future recurrence of haemorrhoids or prolapse.
Laser treatment
Laser treatment has become popular with patients over the course of the past few years. However patients tend to have a science fiction image of laser treatment, imagining that doctors use lasers to vaporize those alien haemorrhoids in an instant, without any damage to the good guys whatsoever. The truth is that while laser can be used for vaporization of the tissues overlying the haemorrhoids, resulting in an ulcer and fixation (in early small internal haemorrhoids) it is mostly used as knife for performing an operation (haemorrhoidectomy). This is the usual way of employing laser in treatment of haemorrhoids, simply because most patients who seek advice have big haemorrhoids, which are only suitable for the latter method. There has been unconfirmed claims that it may result in less postoperative pain (although not entirely painless) in many patients. This is unproven
Stapled anopexy (PPH, Stapled Haemorrhoidectomy)
This procedure (Longo, 1993) aims at lifting up the prolapsed anal cushions rather than removing them. It is suitable for many (most) patients with haemorrhoids. It works best in those with circumferential mucosal prolapse, those with prolapsed haemorrhoids & those with bleeding.
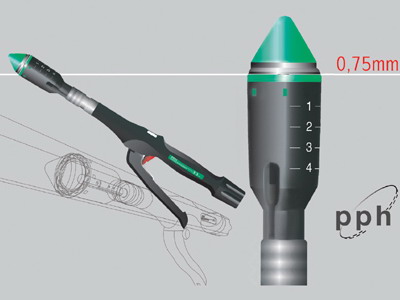 |
| The new PPH03 stapler (Ethicon Endo-Surgery) |
It is not suitable for thrombosed haemorrhoids and is not ideal for patients with large 4th degree haemorrhoids or those with fibrosed anal skin tags
It results in less pain and earlier return to work & social activities.
If this operation is (incorrectly) done low in the rectum / top of anal canal, it potentially can damage anal sensation (if it damages the anal transitional zone, responsible for differentiation between flatus, liquids and solids) or rarely the anal sphincters, affecting continence. There is a very small risk of causing rectovaginal fistulae and very very rarely pelvic sepsis. Sometimes patients may have unexplained anal / rectal pain for sometime following this operation. However, on the whole this is a very safe alternative to traditional haemorrhoidectomy. Lastly, patients who may be practicing anal sex should be warned that the staple line after this operation may interfere with such activities. The procedure is very popular in Europe where it may have been performed in 70-100 thousand patients over the last 10 years